News Story
Addressing liver transplant geographic inequities
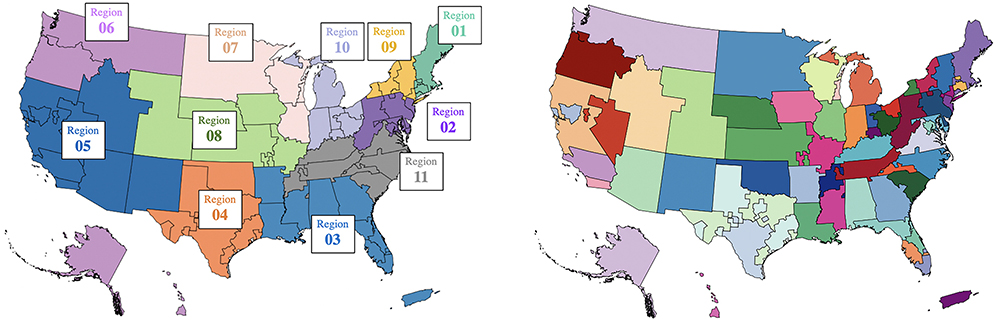
For the purposes of organ allocation, the United States is divided into 11 regions (left) comprising 58 donation service areas (right). Fig. 1 from the paper. [Click image for larger view]
The recent overhaul of the federal policy on allocating deceased donor livers has not significantly improved geographical inequities yet has led to a greater loss in viable organs, according to “Improving Broader Sharing to Address Geographic Inequity in Liver Transplantation,” new research from by University of Maryland faculty and alums. They recommend improving the broader sharing approach outlined in the 2020 policy, known as Acuity Circles, to mitigate inequities across regions of the country; these include variations in transplant rates, patient survival rates, waiting times and organ offers.
The study was written by alum Shubham Akshat (BMGT Ph.D. 2022), visiting assistant professor of operations management at Carnegie Mellon University; S. Raghu Raghavan (BMGT/ISR), Dean's Professor of Management Science and Operations Management; and Liye Ma (BMGT), associate professor of marketing. Akshat was advised by Raghavan as a Ph.D. student; all authors are associated with the Robert H. Smith School of Business.
The paper is forthcoming in the INFORMS journal Manufacturing & Service Operations Management.
“Recent policies are moving toward broader sharing in principle, but the current Acuity Circles policy leads to even lower efficiency,” said Raghavan. “We suggest policymakers move away from the ‘one- size-fits-all’ approach of current policy and focus on a customized approach involving equalizing the organ supply to transplant demand ratios across the transplant centers in the country.”
Liver transplant is the last treatment option for patients with end-stage liver disease. The number of people waiting for a liver transplant, however, greatly exceeds the number of available deceased-donor liver; nearly 1,200 people died in 2021 waiting for a liver transplant. Moreover, there is significant geographical variation across transplant centers across the country, resulting in geographic inequity in terms of access to transplant.
The U.S. government created the Organ Procurement and Transplantation Network (OPTN) in 1984 to coordinate a nationwide transplant system and optimize the use of limited donor organs for transplants. Since 1986, the United Network for Organ Sharing, a nonprofit private organization, has overseen its operations.
A key regulatory framework guiding organ transplantation is the Final Rule, which was adopted in 1998 by the U.S. Department of Health and Human Services and states that policies shall not be based on the candidate’s place of residence. However, disparities in organ access have been a serious issue for more than two decades. In 2012, OPTN’s board adopted a strategic plan that included reducing geographic disparities in accessing transplantation.
For the purposes of organ allocation, the United States is divided into 11 geographic regions, consisting of 58 Donation Service Areas (DSAs). A DSA-based allocation policy was in place from 1989 to February 2020, when it was replaced by the Acuity Circles policy, which provides a one-size-fits-all variant of broader sharing.
In the transplant community, broader organ sharing is believed to mitigate geographic inequity when considering access to organs. In this study, researchers developed a model based on about 40 medical characteristics of patients and donors to analyze allocation policies that differ from current and proposed policies, and to determine whether a better alternative exists.
The model accurately predicts the change in a patient’s organ-offer acceptance probability due to a change in policy. They used data from the Scientific Registry of Transplant Recipients, which includes information on all donors, wait-listed candidates as well as U.S. transplant recipients.
“Our model can be used to provide more accurate policy evaluations to decision makers,” Ma said.
“This model would account for the variation of ‘incidence of disease’ (i.e., demand) and ‘availability of deceased-donor organs’ (i.e., supply), and allow for variations in how broadly a donor hospital shares its organs (i.e., how far it will be shared),” said Akshat, who led the study. “Although this may not sound immediately fair, it results in a policy with greater equity than the current transplant policy.”
This article first appeared in the May 3, 2023 edition of Maryland Today. It was adapted from Carnegie Mellon University and INFORMS news releases.
Additional liver transplant network research by Raghavan and his colleagues
Raghavan and Akshat have previously collaborated on liver transplant network research. In 2020, along with Sommer Gentry (USNA/JHU School of Medicine) they wrote the paper, Fair Liver Transplant Allocation: A Scalable Optimization Model. This work reformulates the current allocation situation as a set-partitioning problem, enabling scaling to more granular geographical units. The model matches supply and demand in a more equitable fashion than existing and proposed policies; and holds significant potential to improve the liver transplantation landscape, potentially saving 340 lives on average over a period of four years.
| Read more about the earlier work here on the ISR website |
Additional links
Published May 4, 2023
Related Stories
Stories / March 31, 2023
When does a package delivery company benefit from having two...
Stories / September 14, 2022
Alum Ahmed Arafa wins NSF CAREER Award

Stories / December 7, 2021
Alumni Profile: Yijie Han

Stories / November 5, 2020
Alumnus Ravi Tandon earns tenure at University of Arizona

Stories / September 14, 2020
S. Raghu Raghavan is PI for NSF project on illicit drug...

Stories / May 14, 2020
Alumnus Rajiv Laroia honored with IEEE Alexander Graham Bell...

Stories / June 22, 2018
Alumna Mingyan Liu named ECE chair at University of Michigan
Stories / May 8, 2018
Alum Mingyan Liu is PI for Multiscale Network Games of...
Stories / February 10, 2017
Alumnus Serban Sabau wins NSF CAREER Award for network research

Stories / April 12, 2016
Alumnus Radha Poovendran is PI for cybersecurity MURI grant
